Events & Promotions
|
|

GMAT Club Daily Prep
Thank you for using the timer - this advanced tool can estimate your performance and suggest more practice questions. We have subscribed you to Daily Prep Questions via email.
Customized
for You
Track
Your Progress
Practice
Pays
Not interested in getting valuable practice questions and articles delivered to your email? No problem, unsubscribe here.
 Jun 08
Jun 0803:00 PM PDT
-04:00 PM PDT
15 Full-length GMAT FE mocks with insightful analytics, weakness diagnosis, and video explanations! Jun 08
Jun 0808:00 PM EDT
-10:00 PM EDT
Master the GMAT with expert live instruction, a personalized study plan, and real-time support. Includes 40 hours of online classes plus 6 months of access to the TTP GMAT OnDemand video course. Mon/Wed June 8, 2026 →August 12, 2026 8:00pm-10:00pm EST Jun 10
Jun 1012:30 AM EDT
-01:30 AM EDT
Thought your job leaves no time for GMAT prep? After multiple GMAT attempts and a demanding consulting job, Kshitij improved to 695 in under 2 months. Learn the mindset shifts, study strategy, and execution changes that made the breakthrough possible. Jun 10
Jun 1006:00 AM PDT
-06:15 PM PDT
Register for the GMAT Club Virtual MBA Spotlight Fair – the world’s premier event for serious MBA candidates. This is your chance to hear directly from Admissions Directors at nearly every Top 30 MBA program..- Jun 10
10:00 AM PDT
-11:00 AM PDT
Scoring 715 on the GMAT Focus Edition requires more than just learning formulas, memorizing concepts, or solving hundreds of questions. In this episode, Nishant shares how he improved his GMAT preparation by focusing on application of concepts, and more.  Jun 11
Jun 1101:30 AM EDT
-02:30 AM EDT
At one point, she believed GMAT wasn’t for her. After scoring 595, self-doubt crept in and she questioned her potential. But instead of quitting, she made the right strategic changes. The result? A remarkable comeback to 695. Check out how Saakshi did it. Jun 11
Jun 1111:00 AM EDT
-01:00 PM EDT
TTP GMAT OnDemand gives serious students 400+ hours of expert video instruction, the full TTP course, AI support, weekly office hours, and a 715+ score guarantee—all built for elite GMAT score improvement.

Kudos
Bookmarks
Evidence-based medicine (EBM) is the explicit, judicious, and persistent use of best-available clinical scientific evidence in medical practice. When EBM is successfully introduced, widely accepted diagnostic or treatment regimens are often found less safe or less effective than alternatives, and then replaced.
The claim that almost all clinicians practice EBM to the extent allowed by available evidence is simply false: there is ample data confirming the striking variations in the rates, within disciplines such as general medicine, that clinicians provide certain proven interventions for patients. The difficulties that clinicians face in keeping abreast of medical advances are obvious when comparing the time required (for general medicine, enough to examine 19 articles per day) with the time available (under an hour a week for doctors in Nation X). However, clinicians who devote their scarce reading time to selective, efficient searches for, appraisals of, and incorporation of the best available evidence can practice EBM.
The claim that almost all clinicians practice EBM to the extent allowed by available evidence is simply false: there is ample data confirming the striking variations in the rates, within disciplines such as general medicine, that clinicians provide certain proven interventions for patients. The difficulties that clinicians face in keeping abreast of medical advances are obvious when comparing the time required (for general medicine, enough to examine 19 articles per day) with the time available (under an hour a week for doctors in Nation X). However, clinicians who devote their scarce reading time to selective, efficient searches for, appraisals of, and incorporation of the best available evidence can practice EBM.

Non-drug treatments require, on average, more skill to implement than do drug treatments.: Yes
Clinicians within certain specialties tend to recommend drug treatments more often than clinicians working within other specialties tend to recommend drug treatments.: No
Clinicians working within general medicine vary considerably in the amount of time they devote to examination of current research.: No
Be sure to select an answer first to save it in the Error Log before revealing the correct answer (OA)!
Difficulty:
 95%
(hard)
95%
(hard)
Question Stats:
29% (03:11) correct 71%
(03:36)
wrong
based on 389
sessions
71%
(03:36)
wrong
based on 389
sessions
History
Date
Time
Result
Not Attempted Yet
For each of the following statements, select Yes if the information provided suggests that the statement would, if true, help explain an aspect of the results given in the graph. Otherwise, select No.
| Yes | No | |
| Non-drug treatments require, on average, more skill to implement than do drug treatments. | ||
| Clinicians within certain specialties tend to recommend drug treatments more often than clinicians working within other specialties tend to recommend drug treatments. | ||
| Clinicians working within general medicine vary considerably in the amount of time they devote to examination of current research. |
ShowHide Answer
Official Answer
Non-drug treatments require, on average, more skill to implement than do drug treatments.: Yes
Clinicians within certain specialties tend to recommend drug treatments more often than clinicians working within other specialties tend to recommend drug treatments.: No
Clinicians working within general medicine vary considerably in the amount of time they devote to examination of current research.: No
A significant number of general practitioners within Nation X have sufficient time for and interest in examining research related to drug treatments.: Two Together
A significant number of general practitioners within Nation X lack sufficient time for and interest in examining research related to drug treatments.: Two Together
General practitioners in Nation X are much more likely to offer drug treatments to their patients than certain non-general-practitioners are.: Other
Be sure to select an answer first to save it in the Error Log before revealing the correct answer (OA)!
Difficulty:
95%
(hard)
Question Stats:
23% (01:20) correct
77%
(01:40)
wrong
based on 441
sessions
History
Date
Time
Result
Not Attempted Yet
Which TWO of the following statements would, if true, together help explain the finding that the author of the EBM tab claims is confirmed by data? Select Two together for the two statements that would clearly contribute to the strength of the explanation. For the remaining statement, select Other.
| Two Together | Other | |
| A significant number of general practitioners within Nation X have sufficient time for and interest in examining research related to drug treatments. | ||
| A significant number of general practitioners within Nation X lack sufficient time for and interest in examining research related to drug treatments. | ||
| General practitioners in Nation X are much more likely to offer drug treatments to their patients than certain non-general-practitioners are. |
ShowHide Answer
Official Answer
A significant number of general practitioners within Nation X have sufficient time for and interest in examining research related to drug treatments.: Two Together
A significant number of general practitioners within Nation X lack sufficient time for and interest in examining research related to drug treatments.: Two Together
General practitioners in Nation X are much more likely to offer drug treatments to their patients than certain non-general-practitioners are.: Other
It addresses a potential objection to EBM by elaborating on an aspect of the definition of EBM stated in the EBM tab.
Be sure to select an answer first to save it in the Error Log before revealing the correct answer (OA)!
Difficulty:
65%
(hard)
Question Stats:
51% (01:34) correct
49%
(01:42)
wrong
based on 370
sessions
History
Date
Time
Result
Not Attempted Yet
If the information given forms a portion of a presentation by an advocate of EBM, which one of the following would most accurately describe the role of the Final Point tab?
| It serves to emphasize the point made in the final sentence of the passage in the EBM tab. | |
| It describes an aspect of one of the difficulties associated with the practice of EBM, discussed in at least one of the other two tabs. | |
| It draws an inference from the relative difficulty of implementing non-drug treatments. | |
| It addresses a potential objection to EBM by elaborating on an aspect of the definition of EBM stated in the EBM tab. | |
| It addresses a potential objection to EBM by expanding on the significance of the study results presented in the graph. |
ShowHide Answer
Official Answer
It addresses a potential objection to EBM by elaborating on an aspect of the definition of EBM stated in the EBM tab.
Attachment:
GMAT-Club-Forum-5mpix15i.png [ 50.57 KiB | Viewed 3979 times ]
Attachment:
GMAT-Club-Forum-5mpix15i.png [ 50.57 KiB | Viewed 3979 times ]
Attachment:
graph.png [ 50.57 KiB | Viewed 4814 times ]
Using official mocks already?
Add GMAT Club Tests for harder practice, analytics, and explanations without overlapping Official Guide or official mock questions.
Try it now →
Try it now →



Kudos
Bookmarks
Let's start by summarizing what each tab is actually saying.
__________________________________________________________________
TAB SUMMARY:
Tab 1 EBM
This tab defines evidence based medicine as using the best available clinical evidence in practice, with good judgment. It argues that it is false that almost all clinicians practice EBM as much as the evidence allows. The tab says data show striking variation in how often clinicians provide proven interventions, even within general medicine. It also explains a key reason this happens. Keeping up with advances would require far more reading time than many doctors have, illustrated by the contrast between the time needed to read many articles per day and the fact that doctors in Nation X have under an hour a week.
Tab 2 Information
This tab describes a review of 80 studies gathered in an EBM focused publication. It gives the study breakdown, 55 single randomized trials and 25 systematic reviews, with roughly half about drug treatments. The key detail is that precisely half of the studies were missing information necessary for clinicians to apply the treatments. When researchers contacted the original scientists, some gave free online access to the missing essentials. Others refused because of concerns about the skill required to carry out the treatments.
Tab 3 Final Point
This tab clarifies that EBM is not cookbook medicine. It anticipates the objection that EBM forces mechanical decision making. It restates that clinical expertise is needed to decide whether evidence applies to a specific patient and how to integrate it.
__________________________________________________________________
Question 1: For each of the following statements, select Yes if the information provided suggests that the statement would, if true, help explain an aspect of the results given in the graph. Otherwise, select No.
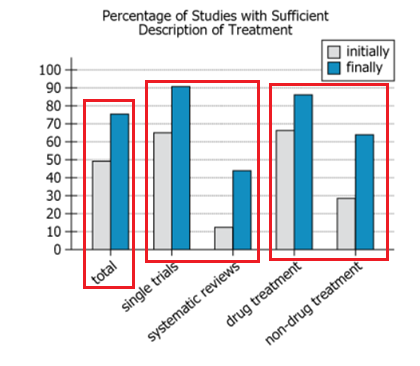
Here, we must decide whether the information, if it were true, would help explain something shown in the graph. The graph is about how often studies include a sufficient description of treatment, comparing what was available initially versus finally after missing details were sought.
• Non-drug treatments require, on average, more skill to implement than do drug treatments.
The Information tab says some scientists were unwilling to provide necessary details because of concerns about “the amount of skill required to carry out the treatments.” If non drug treatments generally require more skill, that would help explain why non drug treatment studies seem to have lower rates of sufficient description, especially at the initial stage.
Answer Yes.
• Clinicians within certain specialties tend to recommend drug treatments more often than clinicians working within other specialties tend to recommend drug treatments.
This does not explain the graph’s pattern. The graph is not about how often clinicians recommend treatments. It is about whether studies describe treatments sufficiently. The tabs do not connect specialty level prescribing differences to missing treatment description in published studies.
Answer No.
• Clinicians working within general medicine vary considerably in the amount of time they devote to examination of current research.
The EBM tab highlights a time shortage problem, but the graph concerns missing treatment details in research reports and what was later obtained from the scientists. Variation in clinicians’ reading time would not explain why the studies initially lacked sufficient treatment descriptions. The Information tab instead points to researcher willingness and skill concerns as the explanation for missing details.
Answer No.
__________________________________________________________________
Question 2: Which TWO of the following statements would, if true, together help explain the finding that the author of the EBM tab claims is confirmed by data? Select Two together for the two statements that would clearly contribute to the strength of the explanation. For the remaining statement, select Other.
Here we must identify two statements that, if both were true, would together help explain the EBM tab’s data confirmed finding. The clearest such finding is that there are striking variations within general medicine in providing proven interventions.
• A significant number of general practitioners within Nation X have sufficient time for and interest in examining research related to drug treatments.
This would explain why some general practitioners can apply evidence based drug interventions.
• A significant number of general practitioners within Nation X lack sufficient time for and interest in examining research related to drug treatments.
This would explain why other general practitioners do not apply that evidence as consistently.
Together A and B create a direct internal split within general medicine. That kind of split is exactly what would help explain “striking variations” within the same discipline.
• General practitioners in Nation X are much more likely to offer drug treatments to their patients than certain non-general-practitioners are.
This compares general practitioners to other clinicians. It does not explain variation within general medicine. So it is weaker for the specific claim in the EBM tab.
Two Together: A and B.
Other: C.
__________________________________________________________________
Question 3: If the information given forms a portion of a presentation by an advocate of EBM, which one of the following would most accurately describe the role of the Final Point tab?
Here, we must identify the role the Final Point tab plays in a presentation advocating EBM.
• It serves to emphasize the point made in the final sentence of the passage in the EBM tab.
Not correct. The Final Point is not mainly reinforcing the time pressure claim. It shifts to clarifying what EBM is not.
• It describes an aspect of one of the difficulties associated with the practice of EBM, discussed in at least one of the other two tabs.
Not correct. The Final Point is not describing a practical hurdle like limited reading time or missing treatment details. It is clarifying the concept.
• It draws an inference from the relative difficulty of implementing non-drug treatments.
Not correct. The Final Point does not compare drug and non drug treatments. That issue belongs to the Information tab.
• It addresses a potential objection to EBM by elaborating on an aspect of the definition of EBM stated in the EBM tab.
Correct. The Final Point expands the definition of EBM given in the EBM tab. The EBM tab says that EBM requires both evidence and clinical expertise. The Final Point clarifies this by explaining that clinicians must judge whether the evidence fits each patient and cannot follow evidence mechanically. This directly elaborates on the definition and answers the “cookbook medicine” objection.
• It addresses a potential objection to EBM by expanding on the significance of the study results presented in the graph.
Not correct. The Final Point does not focus on interpreting the study results. Its main job is to correct a misunderstanding about what EBM means.

GMAT-Club-Forum-jqlubqml.png [ 39.2 KiB | Viewed 5296 times ]
__________________________________________________________________
TAB SUMMARY:
Tab 1 EBM
This tab defines evidence based medicine as using the best available clinical evidence in practice, with good judgment. It argues that it is false that almost all clinicians practice EBM as much as the evidence allows. The tab says data show striking variation in how often clinicians provide proven interventions, even within general medicine. It also explains a key reason this happens. Keeping up with advances would require far more reading time than many doctors have, illustrated by the contrast between the time needed to read many articles per day and the fact that doctors in Nation X have under an hour a week.
Tab 2 Information
This tab describes a review of 80 studies gathered in an EBM focused publication. It gives the study breakdown, 55 single randomized trials and 25 systematic reviews, with roughly half about drug treatments. The key detail is that precisely half of the studies were missing information necessary for clinicians to apply the treatments. When researchers contacted the original scientists, some gave free online access to the missing essentials. Others refused because of concerns about the skill required to carry out the treatments.
Tab 3 Final Point
This tab clarifies that EBM is not cookbook medicine. It anticipates the objection that EBM forces mechanical decision making. It restates that clinical expertise is needed to decide whether evidence applies to a specific patient and how to integrate it.
__________________________________________________________________
Question 1: For each of the following statements, select Yes if the information provided suggests that the statement would, if true, help explain an aspect of the results given in the graph. Otherwise, select No.
Here, we must decide whether the information, if it were true, would help explain something shown in the graph. The graph is about how often studies include a sufficient description of treatment, comparing what was available initially versus finally after missing details were sought.
• Non-drug treatments require, on average, more skill to implement than do drug treatments.
The Information tab says some scientists were unwilling to provide necessary details because of concerns about “the amount of skill required to carry out the treatments.” If non drug treatments generally require more skill, that would help explain why non drug treatment studies seem to have lower rates of sufficient description, especially at the initial stage.
Answer Yes.
• Clinicians within certain specialties tend to recommend drug treatments more often than clinicians working within other specialties tend to recommend drug treatments.
This does not explain the graph’s pattern. The graph is not about how often clinicians recommend treatments. It is about whether studies describe treatments sufficiently. The tabs do not connect specialty level prescribing differences to missing treatment description in published studies.
Answer No.
• Clinicians working within general medicine vary considerably in the amount of time they devote to examination of current research.
The EBM tab highlights a time shortage problem, but the graph concerns missing treatment details in research reports and what was later obtained from the scientists. Variation in clinicians’ reading time would not explain why the studies initially lacked sufficient treatment descriptions. The Information tab instead points to researcher willingness and skill concerns as the explanation for missing details.
Answer No.
__________________________________________________________________
Question 2: Which TWO of the following statements would, if true, together help explain the finding that the author of the EBM tab claims is confirmed by data? Select Two together for the two statements that would clearly contribute to the strength of the explanation. For the remaining statement, select Other.
Here we must identify two statements that, if both were true, would together help explain the EBM tab’s data confirmed finding. The clearest such finding is that there are striking variations within general medicine in providing proven interventions.
• A significant number of general practitioners within Nation X have sufficient time for and interest in examining research related to drug treatments.
This would explain why some general practitioners can apply evidence based drug interventions.
• A significant number of general practitioners within Nation X lack sufficient time for and interest in examining research related to drug treatments.
This would explain why other general practitioners do not apply that evidence as consistently.
Together A and B create a direct internal split within general medicine. That kind of split is exactly what would help explain “striking variations” within the same discipline.
• General practitioners in Nation X are much more likely to offer drug treatments to their patients than certain non-general-practitioners are.
This compares general practitioners to other clinicians. It does not explain variation within general medicine. So it is weaker for the specific claim in the EBM tab.
Two Together: A and B.
Other: C.
__________________________________________________________________
Question 3: If the information given forms a portion of a presentation by an advocate of EBM, which one of the following would most accurately describe the role of the Final Point tab?
Here, we must identify the role the Final Point tab plays in a presentation advocating EBM.
• It serves to emphasize the point made in the final sentence of the passage in the EBM tab.
Not correct. The Final Point is not mainly reinforcing the time pressure claim. It shifts to clarifying what EBM is not.
• It describes an aspect of one of the difficulties associated with the practice of EBM, discussed in at least one of the other two tabs.
Not correct. The Final Point is not describing a practical hurdle like limited reading time or missing treatment details. It is clarifying the concept.
• It draws an inference from the relative difficulty of implementing non-drug treatments.
Not correct. The Final Point does not compare drug and non drug treatments. That issue belongs to the Information tab.
• It addresses a potential objection to EBM by elaborating on an aspect of the definition of EBM stated in the EBM tab.
Correct. The Final Point expands the definition of EBM given in the EBM tab. The EBM tab says that EBM requires both evidence and clinical expertise. The Final Point clarifies this by explaining that clinicians must judge whether the evidence fits each patient and cannot follow evidence mechanically. This directly elaborates on the definition and answers the “cookbook medicine” objection.
• It addresses a potential objection to EBM by expanding on the significance of the study results presented in the graph.
Not correct. The Final Point does not focus on interpreting the study results. Its main job is to correct a misunderstanding about what EBM means.
Attachment:
GMAT-Club-Forum-jqlubqml.png [ 39.2 KiB | Viewed 5296 times ]
General Discussion

Kudos
Bookmarks
I could not understand the answer for question 1.1
as per me it should be "No" because in the case of non drug treatment there is almost 100% increase in the information after sought out indicating that non drug treatment does not not require so much skill whereas in case of drug treatment the increment is very less indicating that the drug treatment requires much more skill. please clarify
as per me it should be "No" because in the case of non drug treatment there is almost 100% increase in the information after sought out indicating that non drug treatment does not not require so much skill whereas in case of drug treatment the increment is very less indicating that the drug treatment requires much more skill. please clarify
Bunuel